Targeted therapy for chronic inflammatory mouth lesions
What it is
Oral lichen planus (OLP) is a chronic inflammatory condition of the mucous membranes inside the mouth. It is thought to be an autoimmune reaction where the body’s immune system attacks mucosal tissues.
OLP often presents as:
- White, lacy patches (reticular type)
- Red, swollen tissue (erythematous type)
- Painful erosions or ulcers (erosive type)
The condition may cause burning, sensitivity to spicy/acidic foods, and oral discomfort. It is non-contagious but often persistent, requiring long-term management.
Topical calcineurin inhibitors (TCIs) such as tacrolimus and pimecrolimus are now widely used in Korea as steroid-sparing therapies. They reduce immune-driven inflammation while avoiding side effects of prolonged corticosteroid use in the oral cavity.
Why it’s done
Topical calcineurin treatment for oral lichen planus is important because:
✔ Symptom relief – Reduces pain, burning, and discomfort when eating.
✔ Improved quality of life – Allows patients to eat, speak, and socialize more comfortably.
✔ Steroid-sparing benefit – Avoids long-term complications of corticosteroids like mucosal thinning and fungal infections.
✔ Chronic disease control – Helps manage flare-ups in recurrent OLP cases.
✔ Cosmetic reassurance – Improves oral mucosa appearance and reduces anxiety.
Alternatives
While TCIs are highly effective, alternative therapies may also be considered.
→ Topical corticosteroids – First-line therapy, effective but risky with long-term use.
→ Systemic corticosteroids – For widespread or severe erosive disease.
→ Immunosuppressive drugs – Azathioprine, cyclosporine, or methotrexate for resistant cases.
→ Retinoids – Topical or systemic vitamin A derivatives, less commonly used due to irritation.
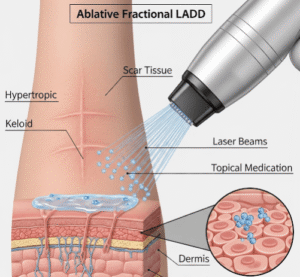
→ Laser therapy – CO₂ or diode lasers for resistant erosive lesions.
→ Observation – For mild, asymptomatic reticular OLP.
In Korea, TCIs are favored for long-term, maintenance-friendly treatment after initial control with corticosteroids.
Preparation
Before starting topical calcineurin therapy, preparation ensures safety and effectiveness.
➤ Diagnosis confirmation – Clinical exam, sometimes biopsy, to rule out dysplasia or oral cancer.
➤ Medical history – Assessment of immune status, allergies, and medication history.
➤ Infection check – Screening for oral candidiasis, which may worsen under immunosuppressive treatment.
➤ Treatment planning – Determining whether tacrolimus or pimecrolimus is more suitable.
➤ Patient education – Clear instructions on application method, possible side effects, and expected timeline of improvement.
How it’s done
Application of topical calcineurin inhibitors for oral lichen planus follows a careful protocol.
➔ Formulation – Tacrolimus or pimecrolimus ointment/gel, sometimes prepared in dental adhesive bases for oral use.
➔ Application –
- Applied directly to lesions with a cotton swab or fingertip.
- Usually 2–3 times daily after meals and oral rinsing.
- Patients avoid eating/drinking for 30 minutes afterward.
➔ Duration – Treatment is continued for weeks to months, with dosage tapered as symptoms improve.
➔ Monitoring – Regular follow-ups to assess improvement and detect complications.
➔ Adjunct care – Korean clinics may combine TCI use with antifungal prophylaxis, soothing oral rinses, and photobiomodulation therapy.
Recovery
Recovery with TCI therapy is gradual but significant.
→ Symptom relief often occurs within 2–4 weeks.
→ Lesions reduce in size, redness, and discomfort with continuous use.
→ Long-term remission is possible with maintenance therapy.
→ Patients regain ability to eat normally, improving nutrition and quality of life.
→ Some cases require repeated or intermittent use during flare-ups.
Complications
While safer than steroids, TCIs are not risk-free.
✔ Transient burning or tingling at application site.
✔ Increased oral candidiasis risk, due to localized immunosuppression.
✔ Pigmentation changes – Rare, but possible with prolonged use.
✔ Potential systemic absorption – Though minimal, long-term monitoring is advised.
✔ Malignancy risk debate – Long-term use has been discussed in medical literature, but no definitive evidence links TCIs with oral cancer; Korean clinics use them with strict follow-up.
Treatment options in Korea
Korea offers specialized care for oral lichen planus with advanced therapies.
➤ Multidisciplinary clinics – Dermatologists, oral medicine specialists, and dentists collaborate for holistic care.
➤ Customized TCI formulations – Many Korean pharmacies prepare dental adhesive pastes with tacrolimus for prolonged contact.
➤ Adjunctive antifungal support – Proactive use of antifungal rinses or lozenges to prevent candidiasis.
➤ Integration with laser therapy – Resistant erosive lesions are treated with low-level laser or CO₂ laser therapy alongside TCIs.
➤ Patient education programs – Detailed instructions and support for long-term self-care.
➤ International patient care – Bilingual consultations, digital follow-ups, and treatment kits for medical tourists.
➤ Research focus – Korean dermatologists and oral medicine researchers actively publish studies on safe long-term use of TCIs in OLP, making Korea a global leader in this field.
By choosing TCI-based oral lichen planus treatment in Korea, patients benefit from advanced formulations, world-class expertise, and integrated oral-dermatology care, ensuring safer long-term disease management.