What it is
➝ Furunculosis is a deep bacterial infection of the hair follicle, usually caused by Staphylococcus aureus, leading to painful, red, swollen nodules filled with pus.
➝ When multiple furuncles cluster, it is called a carbuncle.
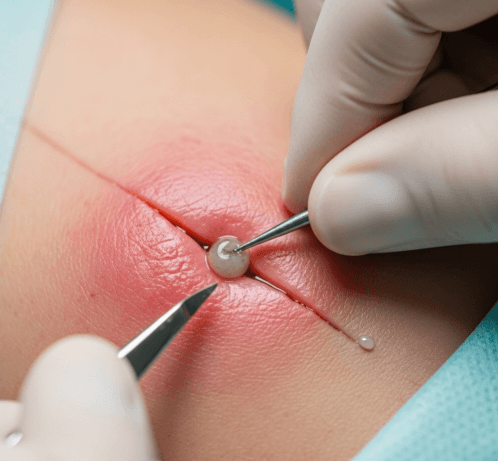
➝ The standard treatment for large, fluctuant, or painful lesions is incision and drainage (I&D), a minor surgical procedure that releases pus, reduces pressure, and speeds healing.
➝ In Korea, incision and drainage is performed widely in dermatology and surgical clinics under sterile conditions, often combined with systemic or topical antibiotics.
Why it’s done
→ To remove pus and necrotic tissue, which antibiotics alone cannot adequately penetrate.
→ To relieve pain, swelling, and tension caused by pus accumulation.
→ To prevent spread of infection to surrounding tissue or into the bloodstream.
→ To promote faster healing and recovery compared to conservative measures.
→ In Korea, I&D is considered the first-line procedure for large or persistent furuncles.
Alternatives
→ Conservative management: Warm compresses to promote spontaneous drainage in small lesions.
→ Antibiotics: Oral or topical therapy for multiple or recurrent furuncles, but less effective without drainage in large abscesses.
→ Laser or surgical excision: Occasionally used for chronic, recurrent furunculosis.
→ Decolonization strategies: For recurrent cases, mupirocin nasal ointment and antiseptic washes to eradicate staphylococcal carriage.
Preparation
→ Clinical examination to confirm fluctuant abscess suitable for drainage.
→ Patients are counseled about the procedure, aftercare, and risk of recurrence.
→ The skin is cleaned with an antiseptic solution (chlorhexidine or povidone-iodine).
→ Local anesthesia (lidocaine injection) is usually given to numb the area.
→ In Korea, many clinics use digital wound documentation systems to monitor healing progress.
How it’s Done
→ A small incision is made over the most fluctuant point of the furuncle.
→ Pus is gently expressed, and loculations may be broken with blunt instruments.
→ The cavity may be irrigated with sterile saline to clear debris.
→ A small sterile dressing or gauze is applied. Sometimes a short-term wick or drain is inserted if the cavity is deep.
→ Antibiotics may be prescribed if there are multiple lesions, systemic symptoms, or risk factors (diabetes, immunosuppression).
→ In Korean practice, wound care often includes antibacterial ointments, hydrocolloid dressings, and regular follow-up.
Recovery
→ Pain relief is usually immediate once pus is drained.
→ Most patients recover within 7–10 days, depending on the size of the lesion.
→ Daily dressing changes and hygiene are important to prevent reinfection.
→ Full healing occurs with minimal scarring if wounds are managed properly.
→ Patients with recurrent furunculosis may need further evaluation for staphylococcal carriage, diabetes, or immune compromise.
Complications
→ Local recurrence if bacteria remain in the skin or follicle.
→ Scarring or pigmentation changes, more common if the lesion is large.
→ Secondary infection if wound care is inadequate.
→ Rare systemic spread leading to cellulitis or sepsis in vulnerable patients.
Treatment Options in Korea
→ Korean dermatology and surgical clinics frequently perform incision and drainage for furunculosis as an outpatient procedure.
→ Many hospitals combine I&D with short courses of oral antibiotics in high-risk patients.
→ For recurrent furunculosis, Korean doctors often recommend nasal mupirocin decolonization and antiseptic body washes to prevent staphylococcal re-colonization.
→ Advanced wound care products, such as antimicrobial dressings and hydrogel patches, are commonly used in Korean clinics to speed recovery and reduce scarring.
→ Patient education includes personal hygiene, not squeezing boils at home, and avoiding sharing towels or razors.
→ With Korea’s strong dermatology infrastructure, patients usually receive fast intervention, structured wound care, and follow-up plans that minimize recurrence.