Overview
Polyserositis is a medical condition characterized by inflammation of multiple serous membranes in the body. These membranes include the pleura (lungs), pericardium (heart), and peritoneum (abdomen). The inflammation leads to fluid accumulation in the affected cavities, which can cause chest pain, abdominal discomfort, breathing difficulties, and other systemic symptoms. Polyserositis is often a manifestation of autoimmune, infectious, or malignant diseases and requires thorough investigation to determine the underlying cause.
What is Polyserositis?
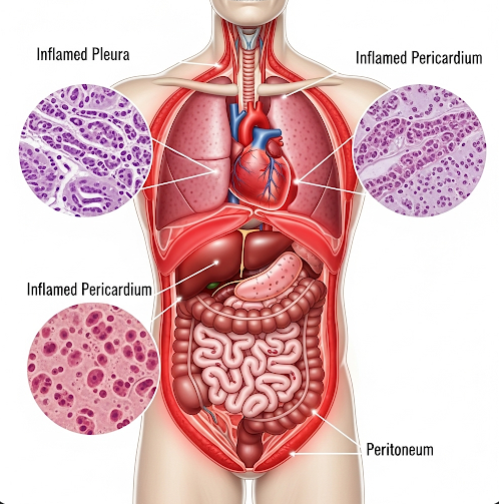
Polyserositis involves simultaneous or sequential inflammation of multiple serosal linings, which are the thin layers of tissue that surround internal organs and secrete lubricating fluid. When these membranes become inflamed, they may produce excess fluid, leading to:
- Pleuritis/pleural effusion (around the lungs)
- Pericarditis/pericardial effusion (around the heart)
- Peritonitis/ascites (in the abdominal cavity)
It is sometimes referred to as “Concato’s disease” when all three serous cavities are involved.
Symptoms
Symptoms of polyserositis depend on the location and extent of inflammation and fluid buildup:
Respiratory symptoms (pleura):
- Sharp chest pain (pleuritic pain)
- Shortness of breath
- Cough
- Shallow or rapid breathing
Cardiac symptoms (pericardium):
- Chest tightness or pain
- Palpitations
- Fatigue
- Low blood pressure or dizziness
Abdominal symptoms (peritoneum):
- Abdominal swelling
- Nausea or vomiting
- Loss of appetite
- Bloating or discomfort
General symptoms:
- Fever
- Malaise
- Weight loss
- Joint pain (if autoimmune-related)
Causes
Polyserositis is usually secondary to an underlying disease. Common causes include:
- Autoimmune diseases
- Systemic lupus erythematosus (SLE)
- Rheumatoid arthritis
- Familial Mediterranean fever (FMF)
- Systemic sclerosis
- Infections
- Tuberculosis (a common cause in endemic areas)
- Viral infections (e.g., Coxsackievirus, HIV)
- Bacterial infections (e.g., pneumonia-related empyema)
- Malignancy
- Lymphomas
- Lung, breast, or gastrointestinal cancers with metastasis
- Kidney or liver failure
- Leading to uremic or hepatic polyserositis
- Post-surgical or post-radiation inflammation
In some cases, the cause may remain idiopathic (unknown).
Risk Factors
Risk factors for developing polyserositis include:
- Autoimmune or connective tissue disease history
- Chronic infections, especially tuberculosis
- Cancer, particularly with serosal involvement
- End-stage renal disease or dialysis
- Chronic liver disease
- Recent cardiac or thoracic surgery
Complications
If left untreated, polyserositis can result in serious complications:
- Cardiac tamponade (life-threatening pressure on the heart)
- Respiratory distress from pleural effusion
- Sepsis or systemic infection
- Chronic organ dysfunction
- Adhesion formation in abdominal or thoracic cavities
- Recurrent effusions
Prompt diagnosis and treatment of the underlying cause can reduce the risk of complications.
Prevention
Prevention depends on managing the underlying conditions and reducing risk factors:
- Early treatment of autoimmune diseases
- Vaccination and infection control, particularly for TB and viral illnesses
- Regular cancer screening in high-risk individuals
- Control of chronic illnesses like kidney and liver disease
- Use of immunosuppressants when appropriate to control autoimmune flare-ups
- Close follow-up after surgery or radiation therapy
Treatment Options in Korea
South Korea offers advanced diagnostic tools and multidisciplinary care for patients with complex inflammatory conditions like polyserositis.
1. Diagnosis
- Imaging: Chest X-ray, echocardiogram, abdominal ultrasound, CT/MRI
- Fluid analysis: Thoracentesis, pericardiocentesis, or paracentesis to test fluid composition
- Blood tests: Inflammatory markers (CRP, ESR), autoimmune panels, kidney/liver function tests
- Microbiology: Cultures for TB, viruses, and bacteria
- Biopsy: In suspected malignancy or unclear diagnosis
2. Medical Management
- Anti-inflammatory medications: NSAIDs or corticosteroids
- Antibiotics or antivirals: If infection is the cause
- Immunosuppressive drugs: For autoimmune diseases (e.g., methotrexate, azathioprine)
- Colchicine: Especially for pericarditis or familial Mediterranean fever
- Chemotherapy or targeted therapy: For malignancy-related cases
3. Surgical/Procedural Intervention
- Drainage of fluid collections (pleural, pericardial, or peritoneal)
- Pericardial window: If fluid around the heart recurs
- Pleurodesis: To prevent recurrent pleural effusion
- Surgical biopsy or tumor resection if malignancy is confirmed
4. Supportive Care
- Hospitalization for severe respiratory or cardiac symptoms
- Nutritional support if gastrointestinal symptoms are present
- Pulmonary and cardiac rehabilitation after fluid removal
5. Leading Hospitals in Korea
Renowned institutions for diagnosis and treatment include:
- Seoul National University Hospital
- Samsung Medical Center
- Asan Medical Center
- Severance Hospital (Yonsei University)
These centers provide:
- Advanced imaging and diagnostics
- Specialists in pulmonology, cardiology, rheumatology, oncology, and infectious diseases
- Integrated, multilingual care for international patients
- Minimally invasive drainage procedures and long-term follow-up