Overview
Squamous cell carcinoma (SCC) is the second most common type of skin cancer, arising from the squamous cells found in the outer layers of the skin. It can also develop in mucous membranes and other areas of the body such as the mouth, esophagus, and lungs. In Korea, the incidence of SCC has been rising, particularly in elderly individuals and those with prolonged sun exposure. Early detection and timely treatment significantly improve outcomes.
What is Squamous Cell Carcinoma?
Squamous cell carcinoma is a type of non-melanoma skin cancer that originates in squamous cells, which form the top layer of the epidermis. SCC is typically caused by DNA damage from ultraviolet (UV) radiation, leading to abnormal cell growth. It usually appears as a scaly red patch, an open sore, or a wart-like growth that may crust or bleed.
While most SCCs are not life-threatening, they can become invasive, spread to other tissues, and cause serious complications if left untreated.
Symptoms
- A persistent, scaly red patch with irregular borders
- A wart-like growth that may bleed or crust
- An open sore that doesn’t heal
- A raised growth with a central depression
- Rough or thickened skin on sun-exposed areas (face, ears, neck, hands)
- In mucosal SCC (e.g., mouth, esophagus): pain, ulcers, or difficulty swallowing
Causes
- Ultraviolet (UV) radiation: From sun exposure or tanning beds
- Human papillomavirus (HPV): Especially for SCC in genital or oropharyngeal areas
- Chronic inflammation or injury: Such as burns, scars, or ulcers
- Exposure to carcinogens: Arsenic, tar, or industrial chemicals
- Weakened immune system: Due to HIV/AIDS, cancer treatment, or organ transplants
- Tobacco and alcohol use: Particularly linked to SCC in the mouth and throat
Risk Factors
- Long-term exposure to sunlight or UV light
- Fair skin, light-colored eyes, and blond or red hair
- Age over 50
- Male gender (slightly higher risk)
- History of precancerous skin lesions (actinic keratosis)
- Personal or family history of skin cancer
- Immunosuppression (organ transplant, chemotherapy)
- Smoking or alcohol use (for mucosal SCC)
Complications
- Local tissue destruction
- Invasion into deeper layers (muscle, bone)
- Lymph node involvement
- Metastasis to distant organs (rare but possible)
- Disfigurement or functional impairment (especially in facial SCC)
- Recurrence after treatment
Prevention
- Avoid prolonged sun exposure, especially between 10 a.m. and 4 p.m.
- Wear protective clothing, hats, and sunglasses outdoors
- Apply broad-spectrum sunscreen (SPF 30 or higher) daily
- Avoid tanning beds and artificial UV exposure
- Regularly check your skin for changes or new lesions
- Treat precancerous lesions (actinic keratoses) early
- Maintain a healthy immune system
- Quit smoking and limit alcohol intake
Treatment Options in Korea
Korea offers advanced and comprehensive care for SCC through its dermatology and oncology departments in public and private hospitals.
Diagnosis:
- Clinical skin examination
- Dermoscopy
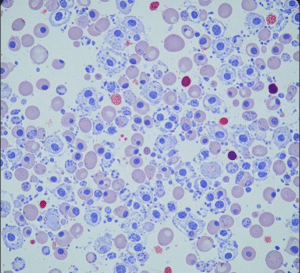
- Skin biopsy (punch or excisional)
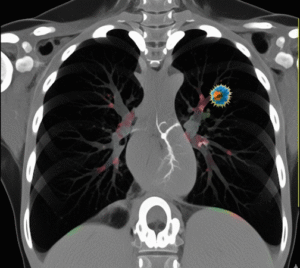
- Imaging (CT, MRI, PET) if spread is suspected
Treatment:
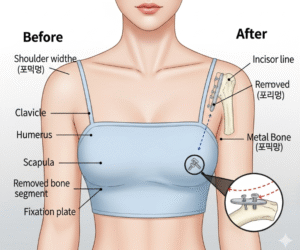
- Surgical excision: Standard treatment with wide margins
- Mohs micrographic surgery: Preferred for facial SCCs or recurrent cases
- Cryotherapy: Freezing precancerous or small superficial SCCs
- Curettage and electrodessication: For small, low-risk SCCs
- Topical treatments: 5-fluorouracil (5-FU) or imiquimod for early lesions
- Radiation therapy: When surgery is not feasible or for advanced cases
- Chemotherapy or targeted therapy: For metastatic or unresectable SCC
Follow-Up Care:
- Regular skin checks every 3–12 months
- Monitoring for recurrence or new skin cancers
- Patient education on sun protection